What if the problem isn’t how clinicians think, but the language we expect them to think in?
I’m Adam Widdison, author of “The Expert Clinician”, where I explore how clinicians really think—and how we can sharpen that thinking in modern practice.
In my last post, The Clinical Paradox, I argued that despite advances in diagnostic technology and AI, the human consultation remains the cornerstone of compassionate and effective care. As medicine becomes more data-driven, there is a growing risk of reducing patients to data points. This makes empathetic, person-centred dialogue more important than ever.
The language we use holds power. It doesn’t just communicate information—it reflects and shapes our beliefs, values, and biases. Clinical language doesn’t simply describe thinking; it influences it.
Medicine prides itself on precision. Yet much of the language used to describe clinical thinking has barely evolved over the past decades. We still teach and document using terminology shaped for a different era—one in which the doctor–patient relationship looked very different. The result is a subtle but persistent mismatch between how clinicians think and how they are expected to describe that thinking.
In this post, I suggest that some of this terminology now limits our perspective—and that small changes in language could better reflect modern clinical practice.
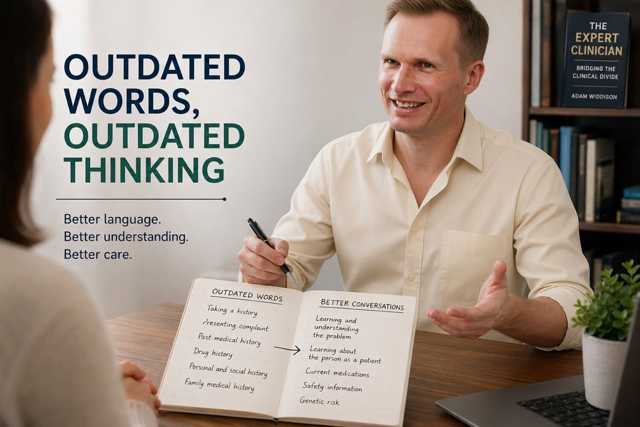
The traditional process of “clerking” begins with “taking a history,” starting with the “presenting complaint,” followed by the “history of the presenting complaint,” “past medical history,” “drug history,” and so on.
This structure is familiar—but familiarity doesn’t guarantee relevance.
Terms like “clerking” and “taking” suggest a passive, administrative role: collecting information, completing a form. But a consultation should be an active process of understanding. It is not about “taking”—it is about learning, interpreting, and making sense of a person’s experience.
Similarly, the term “presenting complaint” carries unintended weight. In everyday language, a “complaint” implies dissatisfaction or grievance. Patients are not complaining—they are seeking help.
A simple shift in language can change perspective:
- “Presenting complaint” → Presenting problem
- “History of presenting complaint” → Learning and understanding the problem
A “problem” invites engagement. It is something worth exploring and addressing. Clinicians are problem-solvers; this framing aligns more naturally with how we think and work.
When we speak of a patient’s “history,” we imply something fixed in the past. But a patient’s experience of illness is not static—it is ongoing.
The consultation is not just about recording what happened. It is about understanding what is happening now, in the context of what has happened before.
Shifting from “taking a history” to learning and understanding the problem places emphasis where it belongs: on interpretation, relevance, and meaning. It recognises that we are not simply gathering facts—we are building understanding.
This becomes even more important when we move beyond the immediate problem.
The traditional “personal and social history” can feel like a checklist. Yet behind these questions is something far more meaningful: understanding the person.
Instead of viewing patients as cases, we should see them as people with problems—individuals navigating life while managing illness.
A small linguistic shift—from “personal and social history” to learning about the person—encourages a deeper, more human perspective. It connects clinical reasoning with the patient’s lived experience.
The same applies to “past medical history.”
Some past events are irrelevant; others are crucial. More importantly, many patients are defined not by past illness but by ongoing conditions they actively manage.
Reframing this as learning about the person as a patient shifts the focus toward:
- meaningful past illness
- current conditions
- ongoing management
- future risk
It reflects how clinicians actually prioritise information in practice.
Even well-established terms like “drug history” carry unintended ambiguity. In modern language, “drugs” are often associated with illicit substance use.
Replacing this with current medications (and, where relevant, previous or future medications) is clearer and more consistent with everyday understanding.
Similarly, “allergies” are often listed as a standalone item, but they represent just one part of a broader concept: patient safety.
A more useful approach is to consider safety information more holistically, recognising risks such as:
- immunosuppression
- bleeding or clotting tendencies
- infection risk to self or others
This reframing aligns better with real clinical decision-making.
Finally, “family medical history” has traditionally been seen as routine—sometimes offering limited insight.
However, in modern practice, this is increasingly about genetic risk. Integrating family history with emerging genetic understanding allows for more proactive, personalised care.
None of these changes is dramatic. But together, they represent a shift in how we think, communicate, and relate to patients.
The words we use are not neutral. They shape our focus, influence our reasoning, and affect how patients experience care.
So perhaps the question is this:
Could the language we’ve never thought to question be quietly limiting the way we practise?
I’d be interested to hear your perspective:
Do you think traditional terminology influences clinical thinking?
In my next blog post, “The Cracks in the Foundation – the Path to Patient-Centred Consultations”, I’ll move beyond language and examine the structure these terms sit within—exploring the broader systemic consequences, and why change is necessary.
Read the full blog and join the conversation 👇
The Cracks in the Foundation – The Path to Patient-Centred Consultations
If these ideas resonate, I explore them further in my book “The Expert Clinician: Bridging the Clinical Divide.” If you want to explore a more effective, flexible, and patient-centred approach to the consultation, I invite you to buy my book. Follow the link to Amazon:

Thoughts? Join the conversation…..